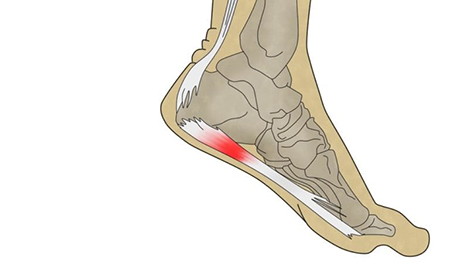
Plantar fascia is pain at the insertion site of the plantar fascia and the calcaneus that may or may not be accompanied by pain along the medial border of the plantar fascia. The diagnosis is primarily clinical. Treatment consists of stretching exercises of the calf muscles and the soft tissues of the sole of the foot, night splints and braces, and shoes with appropriate heel elevation.
Recognized causes of plantar fascia include shortening or contracture of the calf and plantar fascia muscles. Risk factors for this shortening include a sedentary lifestyle, jobs that require sitting, very high or low arches, and chronic use of high-heeled shoes. The condition is also common among runners and dancers, and in people who have to stand or walk on hard surfaces for long periods of time.
Plantar fasciasis may be associated with obesity, RA, reactive arthritis, and psoriatic arthritis. Multiple steroid injections may contribute by causing degenerative changes in the fascia and possible loss of the subcalcaneal fat layer.
The signs and symptoms of plantar fasciitis are characterized by pain at the base of the heel when the foot is supported, particularly upon awakening in the morning; the pain improves within 5-10 minutes and reappears towards the end of the day. It is worse in support and after periods of rest.
Severe acute heel pain, especially with slight local swelling, may indicate an acute fascial tear. Some patients describe a burning or stabbing pain along the medial edge of the sole of the foot when walking.
Treatment of plantar fasciitis will begin with non-invasive treatments such as: bandages, insoles, infiltrations, shock waves, physical therapy. If the plantar fasciitis is chronic and the previous methods have not been effective, surgery should be chosen.